Asthma Medication Administration Form - By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. The osh health care practitioner may decide if the. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath.
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. The osh health care practitioner may decide if the. Assess my child’s asthma symptoms and response to prescribed asthma medicine. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child.
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. The osh health care practitioner may decide if the. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath.

Fillable Online perec.columbia.edusitesdefaultASTHMA MEDICATION
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness.
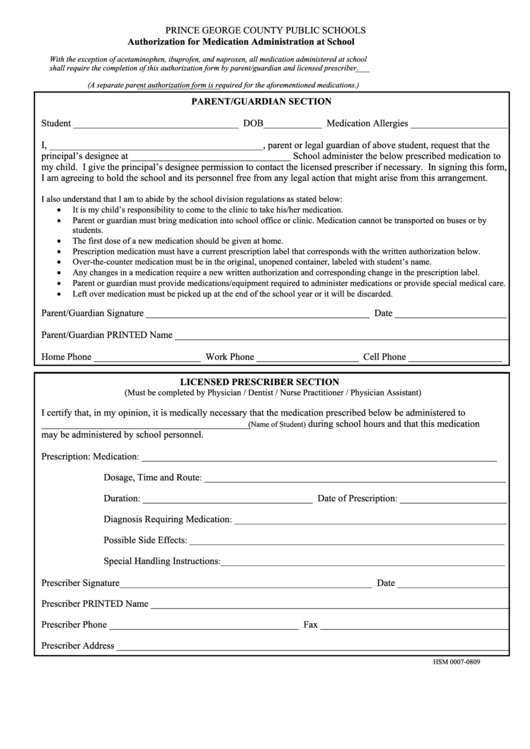
Authorization For Medication Administration At School Form Printable
Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration form (maf), i authorize.
Asthma Medication Administration Form 2024 Jandy Lindsey
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. The osh health care practitioner may decide if the. By signing this medication administration form (maf), i authorize the office.
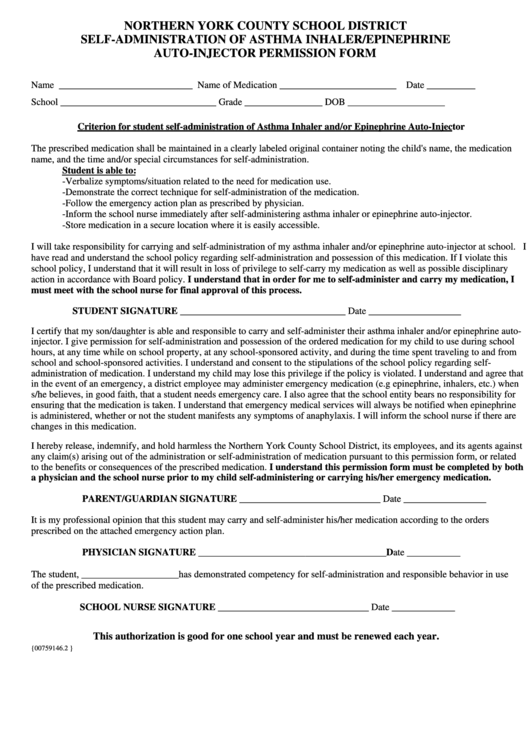
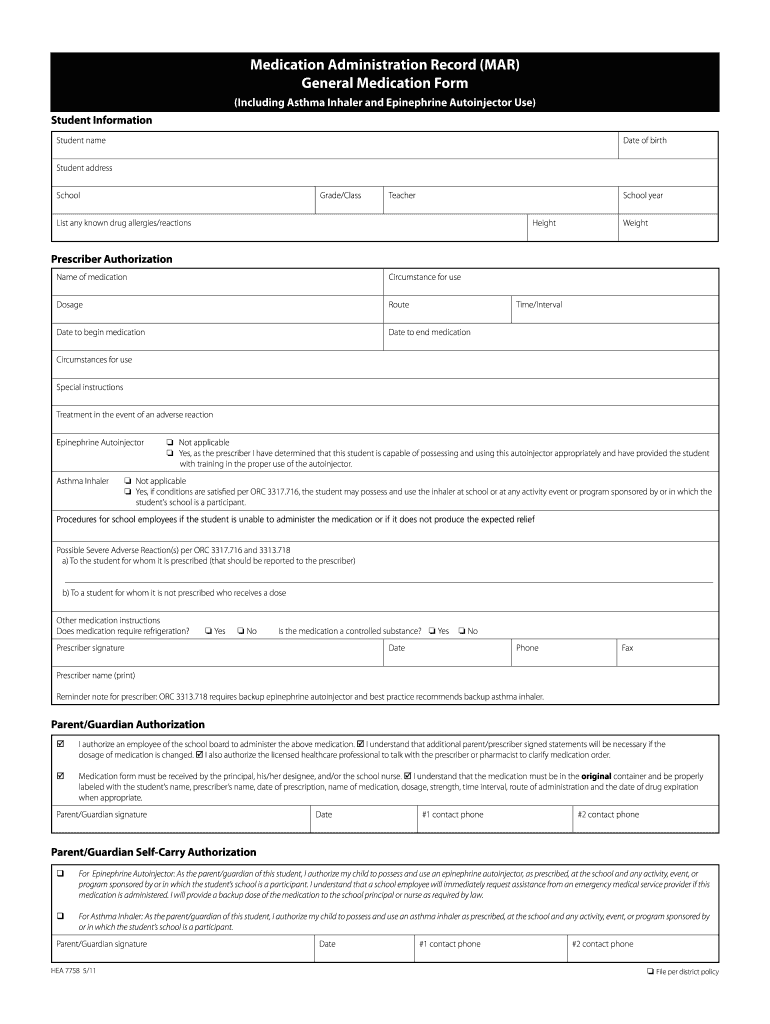
SelfAdministration Of Asthma Inhaler/epinephrine AutoInjector
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to.
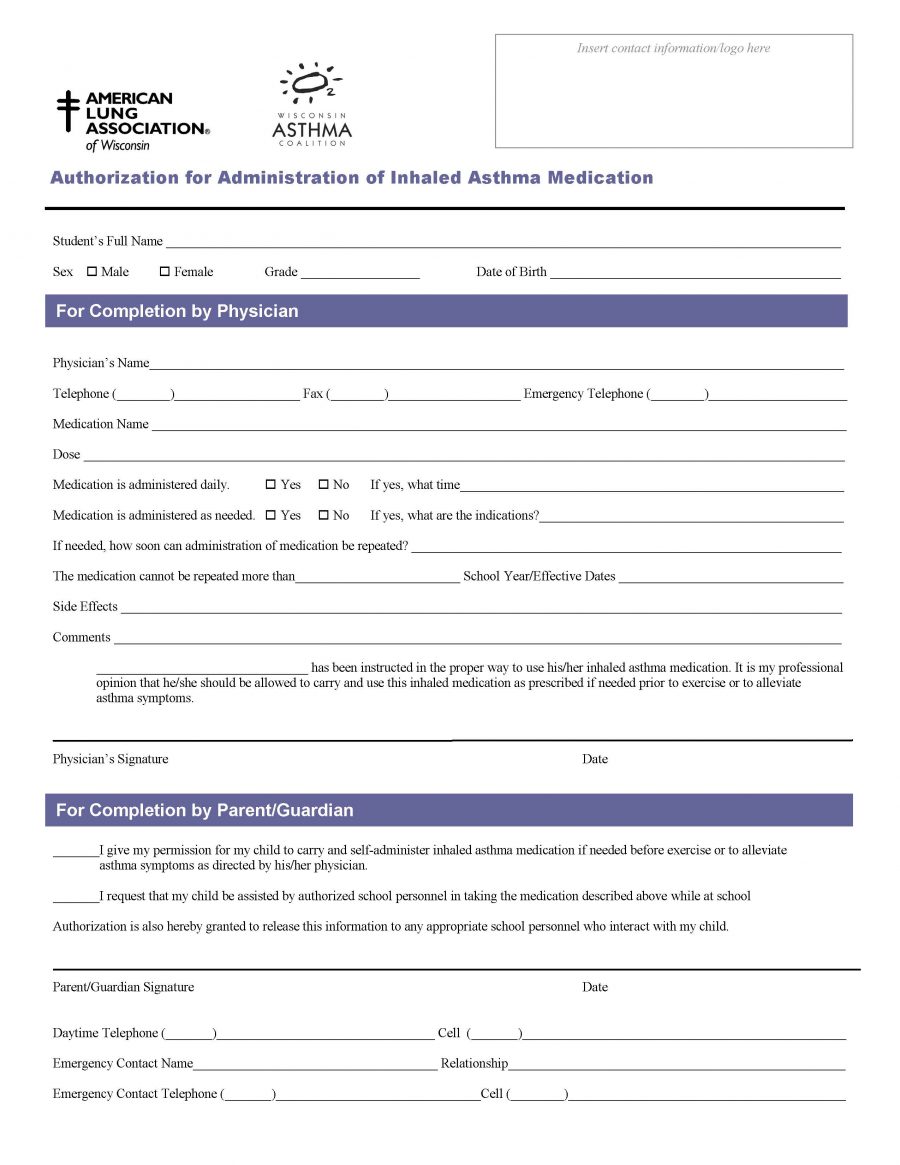
Authorization for Administration of Inhaled Asthma Medication
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. The osh health care practitioner.

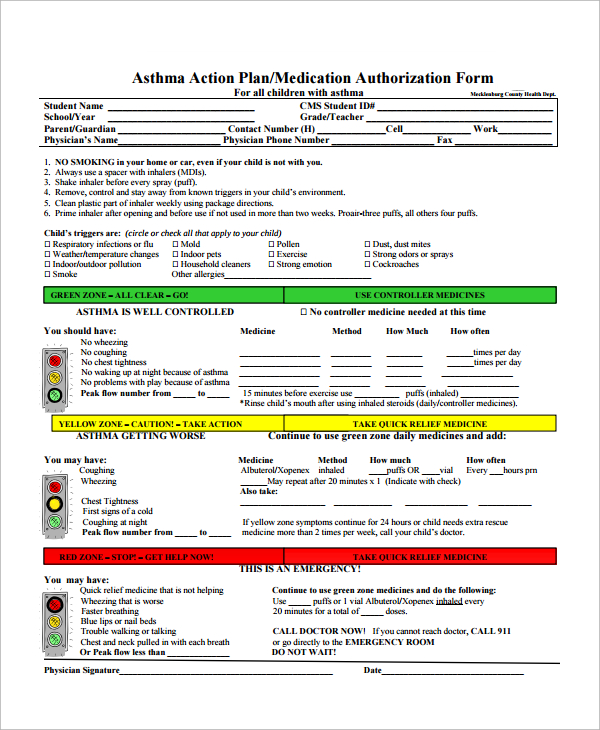
Fillable Online Maryland State School Asthma Medication Administration
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration.
Medication Mar Medication Form Fill Online, Printable, Fillable
The osh health care practitioner may decide if the. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. By signing this medication administration form (maf), i authorize the office.

(PDF) ASTHMA MEDICATION Columbia Universityperec.columbia.edu/files
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. The osh health care practitioner may decide if the. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. By signing this medication administration form (maf),.

Medication Administration Authorization Form 2006 Printable Pdf
By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. The osh health care practitioner may decide if the. Assess my child’s asthma symptoms and response to prescribed asthma medicine..

Asthma medication administration form Fill out & sign online DocHub
Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. The osh health care practitioner may decide if the..
By Signing This Medication Administration Form (Maf), I Authorize The Office Of School Health (Osh) To Provide Health Services To My Child.
Give 2 puffs q 4 hrs prn for coughing, wheezing, tight chest, difficulty breathing or shortness of breath. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child. Assess my child’s asthma symptoms and response to prescribed asthma medicine. By signing this medication administration form (maf), i authorize the office of school health (osh) to provide health services to my child.